Abstract
The suitable placement of a small number of calibrated piezoresistive accelerometer devices may su?ce to assess postures and motions reliably. This ®nding, which was obtained in a previous investigation, led to the further development of this methodology and to an exten- sion from the laboratory to conditions of daily life. The intention was to validate the accel- erometric assessment against behavior observation and to examine the retest reliability. Twenty-four participants were recorded, according to a standard protocol consisting of nine postures/motions (repeated once) which served as reference patterns. The recordings were continued outside the laboratory. A participant observer classified the postures and motions. Four sensor placements (sternum, wrist, thigh, and lower leg) were used. The ®ndings indi- cated that the detection of posture and motion based on accelerometry is highly reliable. The correlation between behavior observation and kinematic analysis was satisfactory, although some participants showed discrepancies regarding speci®c motions. # 1999 Elsevier Science Ltd. All rights reserved.
1. Introduction
The assessment of posture and motion is an essential issue in ambulatory moni- toring because physiological responses, such as changes in heart rate or blood pressure, may result from changes in body position and physical activity. Con- tinuous 24-h recordings of posture and motion can be generally useful in behavior assessment (Fahrenberg & Myrtek, 1996).
The assessment of posture, motion and physical activity will depend on the speci®c aims of a given study. Among these are:.
1. detection of change in body position (e.g. lying supine, sitting, standing) and in body rotation (e.g. during sleep);
2. kinematic analysis, i.e. discrimination of certain patterns of movement (e.g. gait) or of symptoms (e.g. hand tremor, restless legs);
3. discrimination of distinct states (e.g. supine rest, physical exercise);
4. derivation of an overall activity index which provides useful indication of the subject's activity level for the 24-h period;
5. estimation of the momentary metabolic rate (energy expenditure);
6. measurement of relative height of a sensor (e.g. ®nger-cu? for blood pres- sure measurement in relation to the level of the heart);
7. recording of speci®c activities that might invalidate the measurement of other response systems (movement artifacts).
Accordingly, the methods for assessing physical activity vary considerably with respect to type and positioning of sensor, number of recording sites (channels), signal processing (e.g. ®ltering), and statistical procedures.Most investigators use either elec- tromyographic recordings or accelerometer recordings. The registration of the surface electromyogram (EMG) requires the selection of a suitable recording site, preparation of the skin, and application of electrolyte and electrodes allowing for local hydration, as well as ampli®cation, ®ltering, and recti®cation of the raw signal and, ®nally, pro- cessing of the EMG by integration or contour following method (cf. Fridlund & Cacioppo, 1986). Although the EMG is measured in mVolts, an absolute calibration for between-subject designs is not possible because the measurement depends on elec- trode positioning and individual di?erences in morphology and muscular function.
The accelerometer is a widely used method because of its ease of application (Tryon, 1991). However, the available accelerometers di?er in relevant technical aspects even among piezoelectric sensors: general and axial sensitivity (uni-, bi- or tri- axial), frequency range, resonant frequency, damping, and temperature drift. In many instances, such speci®cations are not given by manufacturers. The directional sensitivity is not an all-or-none characteristic but has to be measured by relating signal amplitude and angle of inclination. The available accelerometers, furthermore, di?er in size and mass, durability, and price.
2. Materials and methods
2.1 Participants
In this study, 24 male university students (age range=21±34 years, M=26 years) served as paid voluntary participants. The participants were told that the study would investigate various measures to assess physical activity. Informed consent was obtained.
2.2. Apparatus
The Vitaport 2 (Vitaport EDV Systeme GmbH, Erftstadt, Germany) was used for the multichannel recording. Vitaport 2 is a general purpose digital recorder/analyzer (32 bit microprocessor, 16 MHz) with minimized dimensions and power consump- tion designed for prolonged ambulatory recording. It weighs 700 g. The recorder is carried in a padded bag worn on a belt at the waist. The universal module includes eight analog input channels (16 kHz at 12 bit A/D), with software programmable ampli®er gain, high and low pass ®lter. Storage is available on 16 MByte RAM and 131 MByte Disk. The postprocessing is carried out on Vitagraph Software or add-on analysis programs developed by the user (Jain et al., 1996).
2.3. Accelerometry
The four sensors (IC Sensor Model 3031) were piezoresistive, light-weight, had wide bandwidth (i.e.DCandACresponse), high sensitivity CAN1mV/g (standard range?2 g), a typical accuracy of ?0.2%, and the frequency response was practically linear up to the kHz range. The sensors (supplied by Vitaport, Becker IngenieurbuE ro, Karls- ruhe, Germany), were mounted, 20STx20STx2 mm, weight 4 g, and were equipped by the manufacturer with o?set compensation and temperature drift compensation.
The sensors were calibrated by measuring the signal under controlled inclination, i.e. by rotating the sensor providing a signal output corresponding to +1 and y1 g (the gravitational constant). The DC output is zero when the sensitive axis is parallel to the gravitational axis. The recordings were obtained with a 16 Hz sampling rate and low pass ®ltering at 12 Hz. A higher sampling rate was both unnecessary, and given the limited storage and battery power, undesirable. Four sensors were used:
1. sternum: the sensor that had previously been placed at the regio infra- clavicularis was now placed at the sternum about 5 cm below the jugulum, in order to reduce side e?ects caused by arm movements;
2. wrist (preferred hand): dorsum of the wrist distal from the m. extensor carpi ulnaris;
3. thigh (preferred leg): frontal aspect of thigh, distal from m. rectus femoris;
4. lower leg (preferred leg): frontal aspect of the tibia about 15 cm distal from the patella.
The sensors were fastened with Velcro bands, and the ?exible cables were ®xed to the skin with adhesive medical tape. All connections lead centripetally to the trunk (Vitaport recorder). The sensitive axis of the sensors was roughly perpendicular to the surface, i.e. to the frontal aspect of the sternum, dorsum of the lower arm seg- ment, frontal aspect of thigh, and lower leg segment.
2.4. Procedure
After electrodes and sensors were attached and checked, the following conditions were carried out in a ®xed order:
1. sitting (duration 60 s);
2. standing (duration 60 s);
3. lying supine (duration 60 s);
4. sitting and talking (duration 60 s);
5. sitting and operating PC keyboard (duration 60 s);
6. walking (duration 60 s);
7. stairs up (duration about 40 s); participants were asked to climb stairs (60 steps) at their usual speed in the laboratory building;
8. stairs down (duration about 40 s);
9. cycling (duration about 40 s); participants rode a bicycle around the block.
The record was obtained twice, at the beginning of the recordings and after returning to the laboratory. The participants (and the participant observer, M.S.) spent about 50 min outside the laboratory and engaged in various activities, whereby the observer suggested some kinds of activities in order to obtain a wide range of postures and motions, e.g. upstairs, downstairs, sitting, and lying. How- ever, the participants were relatively free to choose certain settings, e.g. co?ee shop, cafeteria, library, reading a newspaper, conversation, etc. Behaviors were recorded as precisely as possible using a prepared form and stop-watch. A time resolution of at least 3 s was achieved throughout and a segmentation was provided according to the behavior observation, without knowledge of the kinematic analyses.
3. Results
Concerning the accelerometer DC and AC components and throat micro raw signal, substantial di?erences exist?according to the type of physical activity? between conditions. Retest reliabilities of individual measures di?er in size. About 60% of the accelerometer DC and AC variables attain rtt in the range of 0.80±0.99. The reliabilities for certain conditions were obviously dependent on the amount of variance present. For example, during walking the DC components (posture) ster- num, wrist, thigh, lower leg, and head had di?erent rtt values 0.95, 0.41, 0.69, 0.95, and 0.97, respectively, compared to the same components during sitting, 0.73, 0.33, 0.66, 0.29, and 0.94, respectively; the reliabilities for corresponding AC components were 0.99, 0.96, 0.98, 0.98, and 0.98, respectively, during walking and 0.62, 0.25, 0.43, 0.67, and 0.50, respectively, during sitting..
The automatic detection of posture and motion was highly reliable when the method was applied to the recordings obtained for the nine conditions of the second standard protocol. There were only 4.2% misclassi®cations (nine out of 216; see Table 1). These misclassi®cations occurred because of an insu?cient discrimination between walking and walking downstairs (®ve cases), between the three sitting con- ditions (three cases), and between walking and walking upstairs (one case).
Further analyses of discrepancies revealed that elimination of segments shorter than 40 s decreased the percentage of incorrectly classi®ed segments to 69 out of 362.
4.Discussion
As expected, it was more di?cult to detect postures and motions during ambula- tory monitoring outside the laboratory building, where behavior observation was carried out in order to obtain an objective reference. The strategy for detecting behaviors used DC and AC components from four sensors and speech activity, and incorporated standardization and weights. This strategy was satisfactory for the majority of participants and conditions. The percentage of correctly classi®ed seg- ments increased from 67 to 81% when segments with a duration of at least 40 s were analyzed. However, in the case of a number of participants, the discrimination of the three conditions of sitting and the conditions of walking downstairs and walking was particularly unreliable.
It may also be concluded from the present investigation that this methodology is suited to the detection of a variety of motion patterns in the natural setting, pro- vided that the individual's basic patterns are previously assessed under laboratory conditions as a reference. The choice of these tasks is therefore a crucial aspect. The selection used here covered a very large range of postures and movements in daily life. However, it cannot give a complete description because speci®c or mixed behaviors may occur.
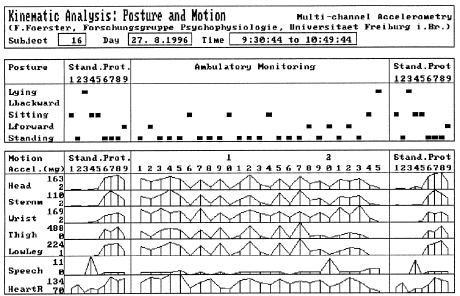
Fig. 1. Kinematic analysis of posture and motion based on calibrated accelerometry for Participant No.
The standard protocol (left-side) consisting of nine conditions was repeated once (right-side). In ambulatory monitoring, 30 segments (duration >20 s) were obtained. Accelerometer recordings from sternum, wrist, thigh, and lower leg, were used for classi®cation of posture and motions. The heavy dashes in the upper section represent change in posture and the polygons in the lower section indicate amount of physical activity (mg) and speech activity (relative units). Heart rate (bpm) was also included in this protocol as an indirect measure of physical activity; however, heart rate was not used at this stage for classi®cation of patterns.
References
1. Bussmann, J. B. J., Tulen, J. H. M., van Herel, E. C. G., & Stam, H. J. (1998). Quanti®cation of physical activities by means of ambulatory accelerometry: a validation study. Psychophysiology, 35, 488±496.
2. Fahrenberg, J., & Myrtek, M. (1996). Ambulatory assessment. Computer-assisted psychological and psychophysiological methods in monitoring and ®eld studies. Seattle, WA: Hogrefe and Huber.с.
3. Fahrenberg, J., MuE ller, W., Foerster, F., & Smeja, M. (1996). A multi-channel investigation of physical activity. Journal of Psychophysiology, 10, 209±217./
4. Fahrenberg, J., Foerster, F., MuE ller, W., & Smeja, M. (1997). Assessment of posture and motion by multi- channel piezoresistive accelerometer recordings. Psychophysiology, 34, 607±612.
5. Foerster, F., & Smeja, M. (1999). Joint amplitude and frequency analysis of tremor activity. Electro- myography and Clinical Neurophysiology, 39, 11±19.
6. Fridlund, A. J., & Cacioppo, J. T. (1986). Guidelines for human electromyographic research. Psycho- physiology, 23, 567±589.
7.Halmos, P. R. (1950). Measure Theory. Princetown, NJ: Van Nostrand.
8.Jain, A., Martens, W. L. J., Mutz, G., Weiu, R. K., & Stephan, E. (1996). Towards a comprehensive.